This article aims to help understand immune problems encountered in ataxia telangiectasia and presented in other sections of this chapter.
Immunity
 Immunity can be defined as the ability to recognize "self", that is to say every single part of my body, and to reject the "non-self", every foreigner who wants to enter it or develop abnormally. We call these intruders antigens.
Immunity can be defined as the ability to recognize "self", that is to say every single part of my body, and to reject the "non-self", every foreigner who wants to enter it or develop abnormally. We call these intruders antigens.
There are three lines of defense:
- the first two are called innate or non-specific because they act regardless of the nature of the aggression.
- the last is called acquired because it is developed according to the type of aggression.
Recognition principle
The self is recognized through the major histocompatibility complex (MHC),called HLA (Human Leukocyte Antigen) in humans: cells have unique surface proteins to differentiate self from nonself.
Note that in humans, the brain has its own immune system separate from the rest of the body.
Types of aggression
Agressions may be:
- Physico-chemical (chemical, climatic, mechanical, ....)
- Due to other organisms (which creates infection) viruses, bacteria, fungi, yeasts, ...
They are permanent.
Defence line 1 : skin and mucous
They both offer a barrier against micro-organisms:
-
The skin is covered with keratin resisting to bacterial enzymes. There are also hair and eyelashes.
-
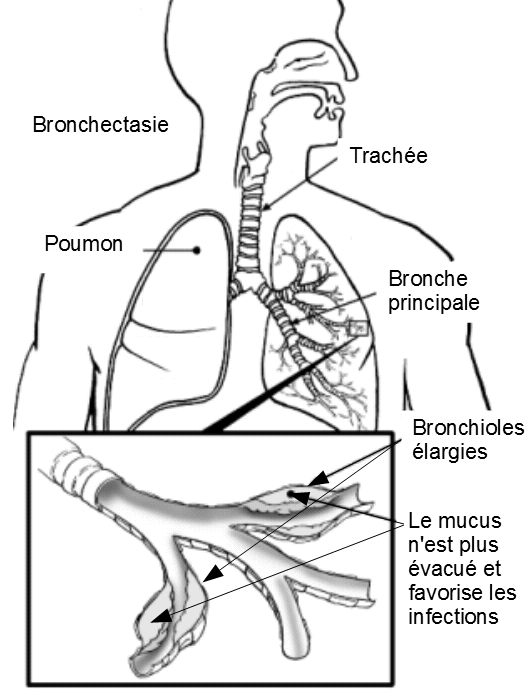
The high impermeability of the very tight mucosal cells protects the respiratory, digestive, respiratory or genito-urinary ways. Some mucous membranes are also covered with a protective film, the mucus, which is evacuated with the foreign bodies "captured" thanks to cilia.
-
In tears and saliva contain lysozyme which destroys the cell wall of many bacteria.
Defence line 2: innate immunity
The second line consists of cellular and chemical defenses:
 Cells have passive defense systems. They are chemical and biochemical enzymes, fatty acids, lactic acid, intestinal flora, pH, etc. ... which create such an hostile environment that number of antigens can't survive.
Cells have passive defense systems. They are chemical and biochemical enzymes, fatty acids, lactic acid, intestinal flora, pH, etc. ... which create such an hostile environment that number of antigens can't survive.
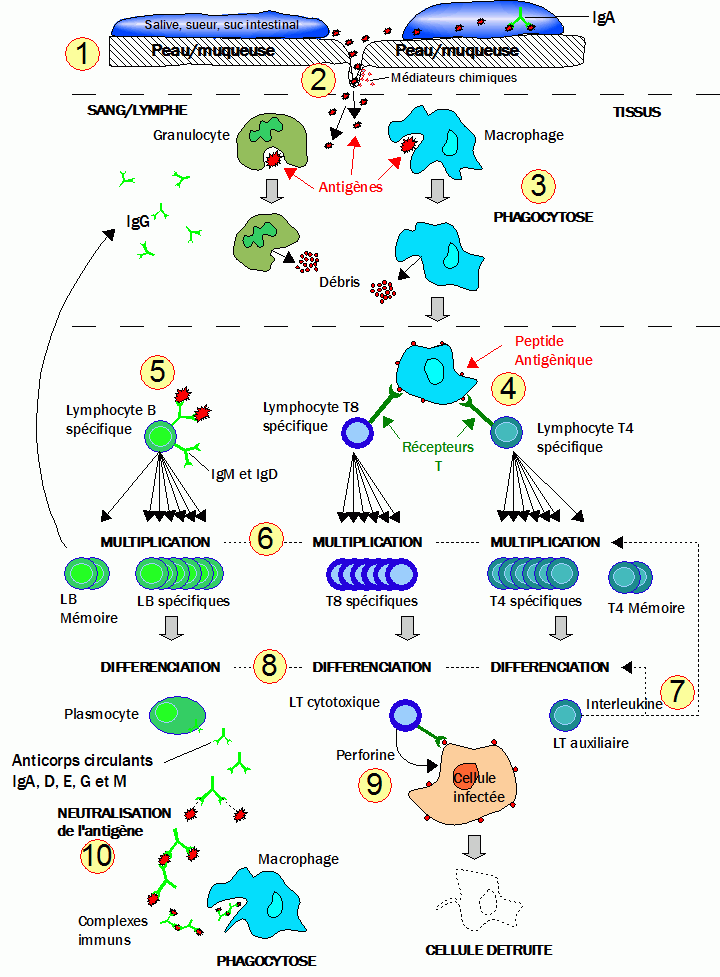
When aggression occurs by injury, damaged cells release chemical mediators that will initiate the inflammatory response: expansion and greater permeability of vessels to rapidly bring the necessary elements to repair and the fight against infections. The area becomes "red" because of the blood flowing.
These chemical mediators will also attract phagocytes (all white blood cells or leukocytes: macrophages, neutrophils and eosinophils), which are responsible for destroying infected cells, microorganisms and foreign substances by eating them (phagocytosis). Note that phagocytes adhere more easily to foreign particles when these are coated with complement proteins and antibodies (see below).
Defence line 3: Specific or acquired immunity
The third line of defense is to develop a personalized response in front of the aggression and memorize it.
This response may take several days before being effective. It is much faster, thanks to the faculty of memory, if the antigen has already tried to invest the body before and is recognized.
Two types of answers are developed from a "specific network", the lymphatic system and the bone marrow:
- Cellular immunity gets rid of the infected cells
- The humoral immunity is to remove free antigens in the body
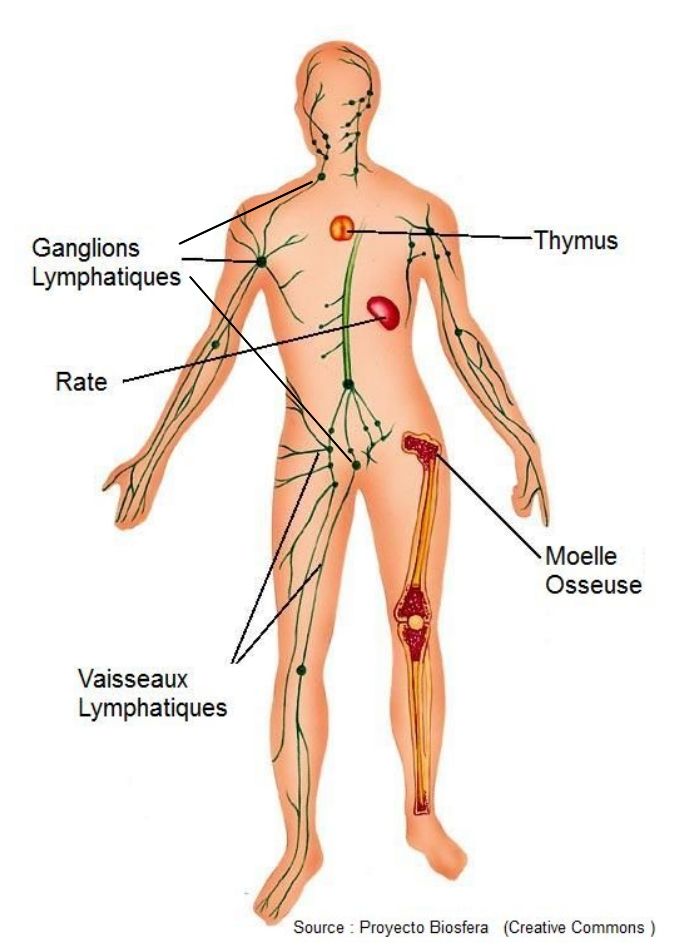
The lymphatic system
- Primary lymphoïd organs: the bone marrow and thymus for the lymphocytes maturation (see below)
- Secondary lymphoid organs: lymph nodes, spleen, tonsils and lymphoid tissues present in the mucous membranes. The lymphatic system, by bringing foreign bodies to these secondary organs, detects, recognizes and activates the mass production of T and B cells needed for the specific response. This explains for example that the closest lymph nodes to the infection swell.
Cellular immunity
The cellular immune system is targetting the body's cells that are infected by viruses or bacteria, and cancer cells.

The action is carried out by T cells that are derived from stem cells from bone marrow and mature in the thymus (T for thymus). There are two families of T lymphocytes:
- Cytotoxic T lymphocytes (TC) test cells surface through their receptors. If they are not recognized, the cell is regarded as foreign and destroyed by chemical perforation of the membrane.
-
{youtubejw}KiLJl3NwmpU{/youtubejw}Helper T cells (TH) interact with macrophages and produce molecules, cytokines (or interleukins) inducing proliferation of B and T lymphocytes and thus a strong immune response.
Humoral immunity
The humoral immune responses can be triggered by:
- Free antigens (antigenic molecules, fragments of membranes)
- Antigens carried by cells (bacteria, infected red blood cells ,...)
These responses involve circulating antibodies: immunoglobulins or antibodies.
What are antibodies? ?
Antibodies are complex proteins for detecting antigens in a specific manner. . These are glycoproteins formed in a Y shape and:
These are glycoproteins formed in a Y shape and:
- Variable parts at the end of each arm of the Y forming the recognition sites of the intruder and allowing the antibody to attach to it.
- Constant parts allowing it to be recognized by the body cells
They are produced by plasmocytes, B lymphocytes that have evolved, marrow stem cells whose maturation also ends in the marrow.
Function of antibodies
Thus equipped, each antibody may:
- Neutralize free antigens:
- Neutralize toxins released by bacteria and thus protect their targets.
- Agglutinate and precipitate antigens (antigenic molecules, fragments of membranes). This option reduces the number of infectious units and, by presenting them in larger complexes and more recognition factors, facilitates their treatment by phagocytosis.
- Clinging to antigens
on the surface of the microorganisms membranes (bacteria, infected red blood cells ...) to:
-
Block the binding capacities of these antigens on the surface of healthy cells or mucous membranes. It is the role of IgA.
-
Make immunocompetent cells (macrophages, NK cell killer ,...) recognize labeled antigens which will be eliminated by phagocytosis. It is opsonization. This usually involves the complement (see below). It is the role of IgG and IgM.
-
Activate the complement
The different antibodies
Antibodies are divided into classes or isotypes, depending on the structure of their constant parts: IgG, IgA, IgM, IgE and IgD.
Moreover, one can classify a population of antibodies according to his ability to recognize one or more antigen binding sites. This is called respectively monoclonal and polyclonal antibodies.
Distribution of the roles of immunoglobulins (Ig) class:
- IgA: mainly in secretions such as saliva, intestinal juices, sweat and breast milk. The main role of IgA is to prevent pathogens from binding to the cell and more specifically to the covering cells of the mucous membranes and the epidermis (outer layer of skin).
- IgM: secreted during the first contact of the organism with an antigen. This is the first class of immunoglobulins released by a variety of white blood cells: plasmocytes. The presence of IgM in the blood indicates a current infection.
- IgE:they are also secreted by plasmocytes in the skin, gastrointestinal tract, tonsils and respiratory tract. This variety of immunoglobulins is connected to mast cells and basophils (white blood cell varieties) by a rod. Upon capture of an antigen, immunoglobulin triggers the release of product involved in the inflammatory response and histamine entering the allergic reaction. IgE concentrations increased in case of severe allergy and parasites are present in the gastrointestinal tract.
- IgG:the most abundant (75 to 80% of circulating antibodies). They are made when a contact with an antigen occurs. They protect the body against bacteria, viruses, and toxins circulating in the blood and lymph. On the other hand, they quickly fix the complement (see above, "complement"). They also participate in the memory response on which is based the mechanism of vaccination. Finally, immunoglobulin G cross the placenta and thus provide the fetus with a passive immunity.
- IgD: most often attached to the surface of B cells where they play a role in antigen receptor. They intervene in the maturation of lymphocytes, that is to say in the mechanism by which these white blood cells become effective.

Complement
Complement is a set of non-specific proteins that are activated in cascade when the antibodies bind to antigens.
This cascade of reactions has four main effects:
- Activate the inflammatory response (see "defence line 2" above)
- Attract phagocytes (eating cells) at the site of infection
- Opsonization of cells presenting antigens (see above: "clinging to antigens).
- Lysis (membrane perforation) of microorganisms marked by the antibodies, in combination with them.
Immune system diseases
The immune system may be faulty:
- by excess when attacking the body's own cells by poor recognition (these are autoimmune diseases).
- by default when allowing cancers and pathogens to develop (in the case of immune deficiency). This is the case in ataxia telangiectasia.
 It's a bit like a construction kit: with the same number of pieces you can make an incredible number of buildings ... And the more you have parts, the more this number increases exponentially.
It's a bit like a construction kit: with the same number of pieces you can make an incredible number of buildings ... And the more you have parts, the more this number increases exponentially.